
They keep catching their foot on the ground as they walk. As they go upstairs, they must lift their knee up higher than expected to clear the step. As they walk, they hear a slapping sound with every other step. What do all these situations have in common? The individuals are most likely suffering from foot drop.
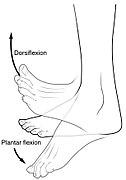
Foot drop is a condition where you have difficulty, or the inability, to bend your ankle up towards your knee. This motion is called ankle dorsiflexion in medical terminology. The main muscle that performs dorsiflexion is the anterior tibialis muscle. This muscle is located just toward the outside of the shin starting below the knee, travels over the top of the ankle, and eventually attaches on the inside of the foot. The common problems associated with this muscle are usually nerve related. So, what sort of conditions affect this muscle? It is helpful to know what nerve innervates the muscle and where that nerve originates from to understand how it can be affected.

The tibialis anterior is innervated by the deep fibular nerve. The deep fibular nerve branches off the common fibular nerve just below the fibular head- which is right below the outside of the knee. The fibular nerve is also referred to as the peroneal nerve. The common fibular nerve starts near the knee when it branches off the sciatic nerve, which is a combination of the tibial and fibular nerves. The sciatic nerve travels up the back of the thigh and to the buttocks, and then close to the spine becomes part of the lumbosacral plexus which is made up of nerves coming from the spinal nerve roots from L4 through S2. The fibular portion of the sciatic nerve is specifically made up from nerves originating from the L4 through S1 nerve root levels.
Now we ask the same question. What conditions affect this muscle and can contribute to foot drop? The most common conditions that cause foot drop are a fibular nerve compromise close to the knee near the fibular head and an L5 lumbar radiculopathy. You can also get foot drop from a sciatic nerve compromise (often in the back of the knee or close to the buttocks from a car accident, fall, surgery), an acquired polyneuropathic process (i.e., diabetic neuropathy), a hereditary polyneuropathy (i.e., Charcot-Marie Toothe), and others (1). We will focus on the two main causes of foot drop; fibular nerve compromise at the knee and L5 radiculopathy, and how you may be able to tell which one you might be suffering from, what you can do about it, and how it may be treated by a doctor.
Fibular Nerve Compromise at the Knee
A fibular nerve compromise at the knee normally involves the common fibular nerve and it is the most common compressive mononeuropathy in the leg (4). The nerve is vulnerable to pressure and compression just past the knee because it is closer to the surface of the skin and is not beneath muscles. Some contributing factors to cause this problem include the following: frequent leg crossing, weight loss, tight casts, space occupying lesions (like a cyst), cancer in the fibular head, recent total knee replacement, and being bedridden (1). With regards to being bedridden, about 10% of patients bedridden in an ICU for more than 4 weeks are expected to develop a problem with the fibular nerve. (1)
L5 Lumbar Radiculopathy
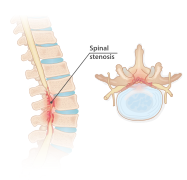
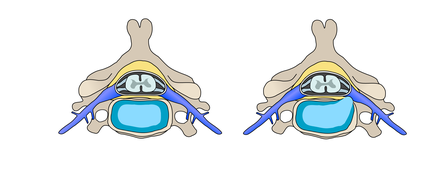
L5 lumbar radiculopathy is the most commonly affected nerve root in the lumbar spine. (2) The nerve root is often compressed because of spinal stenosis or disc herniation. Spinal stenosis is a narrowing of space between vertebrae where the nerve exits the spinal cord. This is related to degenerative changes that may include arthritis, bone spurs, or degenerative disc disease, which decreases the space between vertebral bodies. Stenosis is most commonly found in individuals aged 50 and older. Disc herniations are usually found in younger individuals and occur when compressive forces on the intervertebral discs are too great that the outer, fibrous portion of the disc (annulus fibrosis) gives way to the gel-like substance inside the disc (nucleus pulposus). This is known as disc herniation or disc bulge. In a study from 2019, it was reported that 23% of patients with a disc herniation affecting the L5 nerve root experienced foot drop. (3)
Fibular Nerve vs L5 Lumbar Radiculopathy Signs and Symptoms
So how can someone know which problem may be the cause of their foot drop? Below is a table that will compare the signs and symptoms associated with each condition. This table is not all inclusive, so there may be other symptoms experienced, but these are common symptoms classically associated with these two conditions.
| Fibular Nerve at the Knee | Lumbar Radiculopathy | |
Numbness | On the top of the footWeb spacing between the big and second toes Outside of the lower leg/shin | May not have, but if it does it may be present in the following locations:Top of the footOutside of the lower leg and shinFrom the buttocks down the back of the thigh |
Weakness | Bending the toes up towards the knee (toe extension)Bending the ankle up towards the knee (ankle dorsiflexion)Moving the ankle outwards (ankle eversion) | Bending the toes up towards the knee (toe extension)Bending the ankle up towards the knee (ankle dorsiflexion)Moving the ankle outwards (ankle eversion)Moving the ankle inwards (ankle inversion)Moving the leg/hip out and away from the body (hip abduction) |
Pain | May not have any pain, but if it there is, it may be in the following locations:outside of the knee behind the fibular head- with or without pressure or tapping applied | May not have any pain, but if it there is, it may be in the following locations:Pain in the low backFrom the buttocks down the back of the thigh Outside of the lower leg and shinTop of the foot |
Diagnosis of the Problem
When you see a doctor, they will be considering everything in the table above and will look to see if there is a pattern that fits one of the conditions better than another. They will likely send you for some diagnostic testing to better understand what might be going on. One of the best tests to help differentiate between the two issues is a nerve conduction study (NCS) with electromyography (EMG). The NCS/EMG test can help to determine if it is a nerve problem and to differentiate the location of the problem and understand what muscles or part of the nerve may be affected. Along with an NCS/EMG, the doctor may order an MRI of the lumbar spine to assess for nerve impingement/compression from stenosis or a disc bulge. These two tests will help to cover the most common causes of foot drop along with some additional causes mentioned earlier.
Treatment of the Problem
The treatment of the foot drop will depend on the location of the problem and how long it has been going on. In both cases, a doctor may prescribe an ankle foot orthosis (AFO) to help to keep the foot from flopping down when walking and help to prevent falls due to dragging the toes on the ground. It will also make walking less difficult. The doctor may also prescribe physical therapy for either condition. These are some of the most common conservative treatments.
If the problem is the fibular nerve at the knee they may discuss and recommend surgery to release the nerve from whatever tissues may be contributing to the compression. Treatment for this problem may be a very time sensitive matter to prevent permanent nerve damage from occurring. Other surgical treatments like a tendon or nerve transfer can be performed if the damage to the fibular nerve has been too severe or has been present for a while. (1, 2)
If the problem is in the lower back and your physician is trying to treat it conservatively, they may try an epidural injection along with therapy. If imaging shows a major problem or trials of conservative treatment have failed, the physician may recommend surgery. Depending on the cause of the problem in the back (stenosis or disc), they may recommend a lumbar spinal fusion, a discectomy, or a disc replacement. A neurosurgeon or orthopedic doctor who specializes in spine surgery would be the best choice of physicians to consult.
EMG Solutions specializes in doing NCS/EMG testing, so if you are suffering from foot drop and need a nerve study performed, we at EMG Solutions are here to help so you can get the care and treatment necessary to keep you moving how you want!
Randall Hulet, PT, DPT, ECS