
If I told you a healthy 28-year-old soldier had shoulder pain and could not raise his arm, what causes would come to mind? A rotator cuff tear? A frozen shoulder? Impingement? What would you think if I said he has noticed a protruding shoulder blade during pullups? A long thoracic nerve injury? A brachial plexus compromise? For this patient, the answer was something far less common—an idiopathic spinal accessory nerve injury.
When this young man arrived in my clinic his left trapezius and sternocleidomastoid were atrophied, and he was unable to shrug his left shoulder (see pictures). Interestingly, although CN XI is a purely motor nerve, the patient did have some abnormal sensation over his left trapezius.
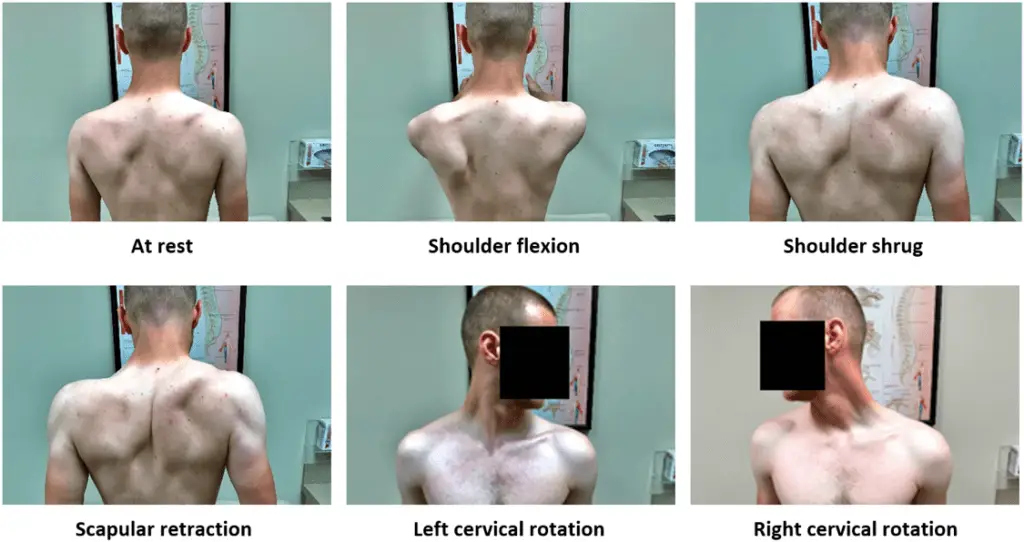
Figure 1: Muscle atrophy and asymmetric movement. Note the left scapular winging with shoulder flexion, the poor elevation with a shoulder shrug, and the absence of a visible sternocleidomastoid with right cervical rotation.
EMG and NCS tests confirmed the patient’s clinical findings. The signal recorded from the left upper trapezius was only 20% as big as the right, and there was no response at all recorded from the left sternocleidomastoid.
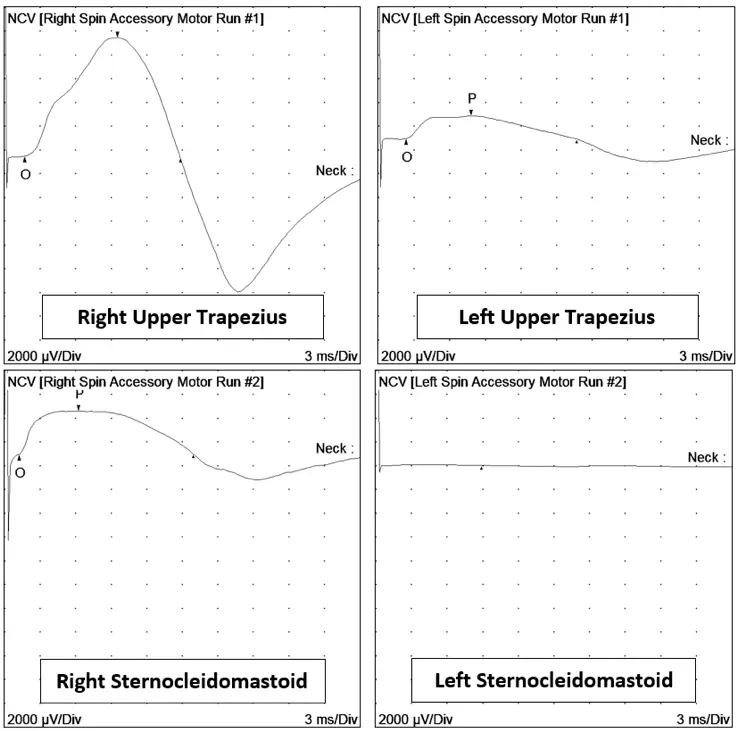
Figure 2: NCS traces from spinal accessory-innervated muscles. Action potential amplitude is dramatically decreased on the affected side, with no recordable response from the left sternocleidomastoid.
Needle EMG cast further light on the case. The affected muscles had abnormalities like decreased insertional activity, complex repetitive discharges, and polyphasic motor unit potentials. All of these indicated that this was not a new injury, but rather had been present for at least several months.
Shoulder pain is a common complaint in the military and is often due to shoulder impingement.(1) Because of this, problems such as a spinal accessory nerve compromise can be missed. Missing a nerve impingement can cause permanent damage and loss of function. One of the most common ways to sustain a spinal accessory nerve injury is due to an excision or biopsy of a lymph node in the surrounding area.(2) Since this patient had neither procedure performed, in is only speculative to conjecture that his nerve compromise may have been due to wearing some sort of backpack.
Do not let this happen to your patients. NCV and EMG studies can help in the diagnosis of a vast array of shoulder problems. Catching a nerve compromise related to Parsonage-Turner syndrome, an axillary nerve, a suprascapular nerve, a spinal accessory nerve, etc. can make the difference between return to function and permanent disability.
(1) Hsiao, M. S., Cameron, K. L., Tucker, C. J., Benigni, M., Blaine, T. A., & Owens, B. D. (2015). Shoulder impingement in the United States military. Journal of Shoulder and Elbow Surgery, 24(9), 1486–1492. doi: 10.1016/j.jse.2015.02.021
(2) Walvekar, R. R., Li, R. J., Gendron, K. B., & Hanby, D. (2020, May 27). Accessory Nerve Injury. Retrieved June 04, 2020, from https://emedicine.medscape.com/article/1298684-overview